.
Chapters
0:00 Introduction
2:44 Causes of Juvenile idiopathic arthritis
3:38 Symptoms of Juvenile idiopathic arthritis
3:55 Diagnosis of Juvenile idiopathic arthritis
5:27 Treatment of Juvenile idiopathic arthritis
Juvenile idiopathic arthritis (JIA), is the most common, chronic rheumatic disease of childhood, affecting approximately one per 1,000 children.[1] Juvenile, in this context, refers to disease onset before 16 years of age, while idiopathic refers to a condition with no defined cause, and arthritis is inflammation within the joint.[2]
JIA is an autoimmune, noninfective, inflammatory joint disease, the cause of which remains poorly understood. It is characterised by chronic joint inflammation. JIA is a subset of childhood arthritis, but unlike other, more transient forms of childhood arthritis, JIA persists for at least six weeks, and in some children is a lifelong condition. It differs significantly from forms of arthritis commonly seen in adults (osteoarthritis, rheumatoid arthritis), in terms of cause, disease associations, and prognosis.
The prognosis for children with JIA has improved dramatically over recent decades, particularly with the introduction of biological therapies and a shift towards more aggressive treatment strategies. JIA treatment aims for normal physical and psychosocial functioning, which is an achievable goal for some children with this condition.[3] Arthritis means inflammation within the joint, and is usually recognised by swelling, pain, stiffness and restricted joint movement. Symptoms of JIA vary from individual to individual. This is mainly because JIA is an umbrella term for several subtypes of JIA, which differ according to the number of affected joints, severity of disease and presence or absence of inflammation in other parts of the body.[citation needed]
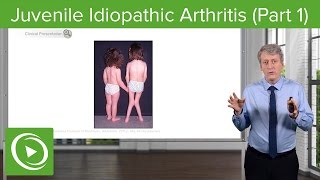
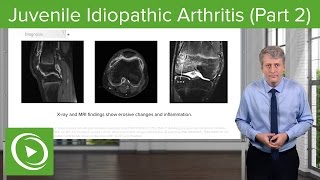
The key clinical feature in JIA is persistent swelling of the affected joints. Any joint can be affected, but large joints such as the knee and ankle are most commonly involved.[4] Involvement of small joints of the hands and feet is more likely when many joints are affected ('polyarthritis'). Swollen joints may also feel warmer to touch. Swelling may be difficult to detect clinically, especially for joints such as those of the spine, sacroiliac joints, shoulder, hip, and jaw; imaging techniques such as ultrasound or MRI can be very useful to identify the inflammation.[citation needed]
Joint pain is an important symptom, although some children experience minimal or no pain with their arthritis.[5] In these children, the first sign of arthritis may be limping, especially in the morning.[5] Young children are often very good at changing how they move when they have joint pain: they learn to move so that it does not hurt. For example, a child will not push up using an inflamed wrist when climbing, instead putting their weight though the forearm. Morning stiffness that improves later in the day is a common feature (this implies inflammatory-type joint pain versus mechanical-type joint pain).[citation needed]
Swelling and pain usually result in limited movement of the affected joints, for example a knee held bent causing a limp, or being unable to make a full fist. Limited movement may reduce a child's ability to fully participate in activities and undertake usual tasks such as those used for self-care. In some JIA subtypes, more non-specific symptoms of being unwell may be present, such as lethargy, fatigue and poor appetite. Children with systemic JIA usually present with fever and a classic rash and may become quite ill. Late effects of arthritis can include joint contractures (stiff, bent joints with loss of movement) due to joint damage; limb length discrepancies and muscle wasting. Children with JIA vary in the degree to which they are affected by particular symptoms.[citation needed]





![BEST 5 Ways to STOP Arthritis Pain [Big 2023 New SECRETS!]](https://i.ytimg.com/vi/5M7ngir46yQ/mqdefault.jpg)



Информация по комментариям в разработке