Tip-129;
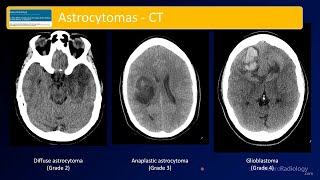
Oligodendroglioma, IDH-mutant and 1p-19q co-deleted, is a diffusely infiltrating glioma with IDH1 or IDH2 mutation and codeletion of chromosome arms 1p and 19q and can be either CNS WHO grade 2 or 3. There is a clear predilection for the frontal lobes, although around 10-15% of cases affect the parietal lobe as in this case. They manifest preferentially in adults, with a median age at diagnosis of 43 years, similar to our case, for patients with histologically defined CNS WHO grade 2 oligodendroglioma and 50 years for those with CNS WHO grade 3 oligodendroglioma. IDH-mutant and 1p-19q co-deleted oligodendrogliomas are rare in children, and you should be cautious when rendering such a diagnosis in the young because of mimics. Seizures are the presenting symptom in approximately two-thirds of cases. Calcifications are commonly seen on CT scans, but they are not diagnostic. MRI typically shows a T1-hypointense and T2-hyperintense mass with indistinct tumor margins. Morphologically, oligodendroglioma cells have uniformly round nuclei that are slightly larger than those of normal oligodendrocytes and show an increase in chromatin density or a delicate salt-and-pepper pattern. The classical typical honeycomb or fried-egg appearance, which, although artefactual due to formalin fixation, is a helpful diagnostic feature, but this is not seen in smear preparations or frozen sections. Oligodendrogliomas typically show a dense network of branching capillaries resembling chicken wire, and in around 50% of cases, calcifications are seen. The tumor typically shows an infiltrative growth pattern, but within the cortex, tumor cells often form secondary structures such as perineuronal satellitosis, perivascular aggregates, and subpial accumulations. More than 90% of IDH mutations in oligodendrogliomas correspond to the recognized IDH1 p.R132H mutation; the remaining tumors carry other IDH mutations, with a higher proportion of IDH2 mutations in oligodendrogliomas than in astrocytomas. There should be a complete deletion of the 1p and 19q arms to render the diagnosis of an oligodendroglioma. Incomplete or partial deletions on either chromosome arm are not compatible with the diagnosis of IDH-mutant and 1p-19q co-deleted oligodendroglioma, but they have been detected in a proportion of IDH-wildtype glioblastomas. Deletions on 9p involving the CDKN2A and/or CDKN2B locus have been associated with CNS WHO grade 3. Histologic mimics include dysembryoplastic neuroepithelial tumor, clear cell ependymoma, neurocytoma, polymorphous low-grade neuroepithelial tumor of the young, and pilocytic astrocytoma, along with the molecularly distinct diffuse gliomas that are characterized by BRAF, FGFR1, MYB, or MYBL1 alterations. Overall, IDH-mutant and 1p-19q co-deleted oligodendrogliomas are associated with favorable response to therapy and median survival times of more than 10 years. Treatment consists of a triad of optimal maximum resection, radiotherapy, and procarbazine, lomustine, and vincristine, PCV, chemotherapy.









Информация по комментариям в разработке