Video transcript :-
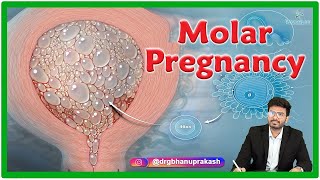
Molar pregnancy, also known as hydatidiform mole, is a type of gestational trophoblastic disease, which includes several disease conditions arising from the placenta.
Some of these diseases include complete and partial moles, placental site trophoblastic tumors, choriocarcinomas, and invasive moles.
The uniqueness of the disease is that the tumor originates only from gestational tissue, rather than from maternal tissue.
Hydatidiform moles are categorized as complete and partial and are usually considered the noninvasive form of gestational trophoblastic disease.
Although they are said to be benign, they have premalignant characteristics and can become malignant and invasive.
Out of the 2 types, complete mole is the most common type and does not contain fetal parts, whereas in a partial mole there might be identifiable fetal residues.
Complete moles are typically diploid, which means they contain 46 chromosomes, whereas partial moles are triploid, which means they have 69 chromosomes.
Complete moles secrete lager amounts of the human chorionic gonadotropin, or HCG, which is one of their main characteristics.
In about 90% of complete moles, the karyotype is 46, XX, and the remaining 10% is 46, XY.
It arises when an enucleated egg is fertilized either by two sperms or by a haploid sperm that then duplicates and therefore, only paternal DNA is expressed.
In partial moles however, 90% of the time the karyotype is triploid and either 69, XXX or 69 XXY.
This happens when a normal sperm subsequently fertilizes haploid ovum duplicates and or when two sperms fertilize a haploid ovum.
Therefore, in partial moles, both maternal and paternal DNA is expressed.
Thanks to the advent of ultrasonography, most moles are now diagnosed in the first trimester before the onset of the classic signs and symptoms.
If present, the most common symptom of a complete mole is vaginal bleeding in the first trimester, which is usually due to the molar tissue separating from the decidua, resulting in bleeding.
Vaginal bleeding is characteristically described as having a "prune juice" appearance.
The patient may also complain of severe nausea and vomiting secondary to extremely high levels of HCG.
Some patients may also have symptoms of hyperthyroidism, including tremors, increased sweating, and diarrhea, due to high levels of circulating HCG.
Patients with partial mole do not have the same clinical features as those with complete mole.
These patients usually present with signs and symptoms consistent with an incomplete or missed abortion, including vaginal bleeding and absence of fetal heartbeat.
In addition to that, in a complete mole, the uterus is usually larger than the expected gestational date of the pregnancy, whereas, in partial moles, the uterus can be smaller than the suggested date.
When a pregnant woman presents with vaginal bleeding, a serum quantitative HCG test should be performed.
Complete moles tend to have very high levels of serum hCG, typically greater than 100,000, whereas partial moles may be within the normal range for gestational age or even lower than expected.
The imaging of choice in a suspected hydatidiform mole is a pelvic ultrasound.
In a complete mole, the ultrasound findings include a heterogeneous mass in the uterine cavity with multiple anechoic spaces, referred to as a "snowstorm" appearance.
In a partial mole, there may be a viable fetus with amniotic fluid.
And the placenta may be enlarged with cystic spaces.
Other essential investigations include a complete blood count to look for anemia and thrombocytopenia.
Blood grouping and rhesus antibody screening.
Serum electrolyte levels.
Thyroid panel if hyperthyroidism is suspected.
Liver enzyme levels.
Urinalysis.
And coagulation profile.
If a molar pregnancy is diagnosed, the next step is typically a CT scan and PET scan to stage the disease.
When the patient presents to the emergency department, initial stabilization if unstable is mandatory.
Once the patient is stabilized, emergency consultation of an obstetrician is essential.
Evacuation of the uterus by dilation and curettage is always necessary.
In patients with advanced maternal age typically greater than 40 years old and those who have completed childbearing, hysterectomy is often performed instead of a Dilation and curettage.
#medtoday #molarpregnancy #mole #hydatidiformmole #completevspartialmole #healtheducation #medicaleducation #medicalknowledge #gynecologist #obstetrics #gyn
molar pregnancy,signs of molar pregnancy,ultrasound,molar pregnancy treatment,molar pregnancy causes,what is a molar pregnancy,molar pregnancy symptoms,partial molar pregnancy,complete molar pregnancy,what causes molar pregnancy,what is molar pregnancy,symptoms of molar pregnancy,molar pregnancy signs,molar pregnancy risks,molar pregnancy cause,cause of molar pregnancy,treatment of molar pregnancy,molar pregnancy usmle,usmle,neet pg,obg,obgyn,obg lectures






Информация по комментариям в разработке