Dr Michelle Kittleson shares noninvasive monitoring strategies for heart transplant rejection.
https://www.medscape.com/viewarticle/...
TRANSCRIPT
Hi. I'm Michelle Kittleson. I'm a heart failure transplant cardiologist and professor of medicine at Cedars-Sinai in sunny Los Angeles, California. I'm delighted to have this opportunity to present a commentary on noninvasive surveillance for heart transplant rejection.
As you may know, the endomyocardial biopsy has been the gold standard for the diagnosis of heart transplant rejection since first pioneered by surgeon Dr Philip Caves and pathologist Dr Margaret Billingham at Stanford in the early 1970s. Interestingly, the bioptome was actually developed about a decade earlier in Japan but was never used in heart transplant recipients. Dr Caves obtained the bioptome from Japan and improved the design using a canine model of heart transplantation. Dr Billingham prepared the biopsy samples and cataloged the pathologic findings, and the field of heart transplantation was born.
Although the endomyocardial biopsy is the gold standard, it's not perfect. It's limited by the associated adverse-event profile, lack of portability, patient discomfort, and low concordance of rejection grading by different observers.
There are other reasons to investigate noninvasive strategies for rejection surveillance. Given the low incidence of asymptomatic rejection, a sensitive surveillance strategy with a high negative predictive value may minimize the number of biopsies needed. A contemporary surveillance strategy should also permit early detection of rejection as compared with the histopathologic changes that represent more advanced stages of immune activation. Blood-based assays also avoid sampling error and interobserver variability grading.
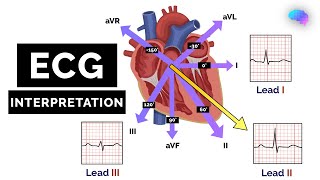
Many of these noninvasive methods have been evaluated, including parameters from electrocardiography, echocardiography, cardiac magnetic resonance imaging, positron emission tomography, as well as biomarkers such as troponin and brain-type natriuretic peptide. However, all of these methods offer limited sensitivity and specificity.
What Is the Noninvasive Approach?
The two most promising noninvasive alternatives to the endomyocardial biopsy include assessment of peripheral gene-expression profiling and donor-derived cell-free DNA. Let's talk about gene-expression profiling first. It quantifies the expression of 11 genes in peripheral blood, mononuclear cells, that are involved in lymphocyte activation, cell migration, T-cell priming, hematopoietic proliferation, steroid sensitivity, and platelet activation pathways.
An activation score was created from the CARGO study to distinguish between moderate and severe acute cellular rejection and quiescence. Use of gene expression profiling in the IMAGE study reduced the number of endomyocardial biopsies performed without an increase in serious adverse events. This is commercially available with the AlloMap assay, and it has an approximately 99% negative predictive value for acute cellular rejection with the AlloMap assay.
Nonetheless, let's talk about pitfalls. Number one, there are pitfalls to interpretation of the findings. You can't interpret an AlloMap gene-expression profiling assay accurately if there's been a recent blood transfusion, or if steroids with 20 mg or higher of prednisone have been administered. Infections can also affect interpretation of results. There are also limitations in that it offers limited positive predictive value, and it was not designed to assess for antibody-mediated rejection (AMR), a major barrier, as treatment, surveillance, and prognosis of AMR differ greatly from those of acute cellular rejection (ACR).
Now let's talk about donor-derived cell-free DNA. The discovery of cell-free DNA dates back to 1948, when it was identified in the sera of patients with cancer. The significance of this observation went unrecognized for decades, although with advances in genetic sequencing, cell-free DNA is now a biomarker for prenatal testing and cancer.
In organ transplantation, donor-derived cell-free DNA was proposed as a noninvasive indicator of graft injury based on the hypothesis that acute rejection causes cell death in the allograft, which leads to increased levels of donor-derived cell-free DNA in the blood of transplant recipients. However, early technologies to quantify donor-derived cell-free DNA in transplant recipients were costly and often impractical, requiring either sex mismatch between donor and recipient, use of the Y chromosome to distinguish donor from recipient DNA, or previous genotyping of the donor and the recipient.
https://www.medscape.com/viewarticle/...









Информация по комментариям в разработке