The three degrees of AV nodal blocks, Mobitz type I and type II.
Purchase a license to download a non-watermarked version of this video on AlilaMedicalMedia(dot)com
Check out our new Alila Academy - AlilaAcademy(dot)com - complete video courses with quizzes, PDFs, and downloadable images.
©Alila Medical Media. All rights reserved.
Voice by: Sue Stern.
All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition.
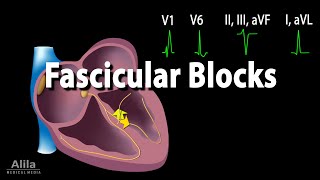
Heart block is a group of diseases characterized by presence of an obstruction, or a “BLOCK” in the heart electrical pathway. A block may slow down the conduction of electrical impulses, OR, in more severe cases, completely stop them. Heart blocks are classified by location where the blockage occurs. Accordingly, there are: SA nodal blocks, AV nodal blocks, intra-Hisian blocks, bundle branch blocks and fascicular blocks.
Of these, AV nodal blocks, or AV blocks, are most clinically significant. In fact, very commonly, the term “heart block “, if not specified otherwise, is used to describe AV blocks. In AV blocks, the electrical signals are slow to reach the ventricles, or completely interrupted before reaching the ventricles.
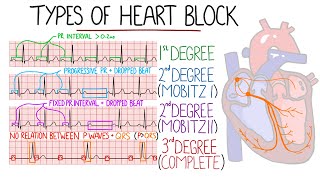
There are three degrees of AV block:
First-degree AV block: the electrical signals are SLOWED as they pass from the SA node to the AV node, but all of them eventually reach the ventricle. On an ECG, this is characterized by a longer PR interval of more than 5 small squares. First-degree AV blocks rarely cause symptoms or problems and generally do NOT require treatment.
Second-degree AV blocks are divided further into type I and type II:
In type I, the electrical signals are delayed further and further with each heartbeat until a beat is missing completely. On an ECG, this is seen as PROGRESSIVE prolongation of PR interval followed by a P wave WITHOUT a QRS complex. This is known as a “blocked” P wave or a “dropped” QRS complex. The cycle then re-starts over. As this usually repeats in regular cycles, there is a fixed ratio between the number of P waves and the number of QRS complexes per cycle. The number of QRS complexes always equals the number of P waves MINUS one. In this example, there are four P waves for every three QRS complexes. This is a “4 to 3” heart block. Second-degree type I blocks are usually mild and no specific treatment is indicated.
In type II second degree blocks, some of the electrical signals do NOT reach the ventricles. On an ECG, this is seen as intermittent non-conducted P-waves. The PR interval, however, remains CONSTANT in conducted beats. In majority of cases, the successfully conducted QRS complexes may appear broader than usual. In some type II blocks, there is a fixed number of P waves per QRS complex. In this example, there are three P waves for every QRS complex and the condition is described as “3 to 1” heart block. However, as the nature of type II block is unstable, this ratio is likely to change over time. Second- degree type II is less common than second-degree type I but is much more dangerous as it frequently progresses to complete heart block or cardiac arrest. Implantation of an artificial pacemaker is recommended for treatment of this type of AV blocks.
Third-degree AV blocks are also referred to as complete heart blocks. In this condition, NONE of the electrical signals from the atria reach the ventricles. With NO input coming from the atria, the ventricles usually try to generate some impulses on their own. This is known as an “ESCAPE rhythm”. On an ECG, two independent rhythms can be seen: a regular P wave pattern represents atrial rhythm; and a regular, but UNUSUALLY slow QRS pattern represents the escape rhythm. The PR interval is variable as there is NO relationship between the 2 rhythms. Patients with third-degree heart blocks are at high risk of cardiac arrest. They require immediate treatment, cardiac monitoring and pacemaker implantation.









Информация по комментариям в разработке