This is a video on prenatal screening, fetal testing, and other tests and methods of evaluating mom and baby during pregnancy.
I created this presentation with Google Slides.
Images were created or taken from Wikimedia Commons
I created this video with the YouTube Video Editor.
ADDITIONAL TAGS:
Prenatal screening, fetal testing, and other tests during pregnancy
Used in
1st trimester to confirm intrauterine pregnancy, gestational age, singleton vs multiple births
GA by measuring crown-rump-length (CRL), most accurate between 7 and 10 w
3rd trimester to assess fetal well-being with BPP, position/orientation, an/oligo/polyhydramnios
Fetal anemia screen (transcranial doppler) after 20 w
High velocity means baby Bb is low
Cardiotocography for fetal monitoring uses Doppler u/s: see NST, CST, BPP
Benefit: no risk to fetus and no complications
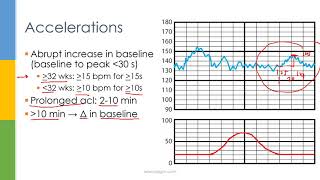
2 15 bpm accelerations lasting 15 sec (15 for 15, or 10 for 10 32 wks)
Baseline heart rate of 110 to 160 bpm
Moderate variability (6-25 bpm)
No late or variable decels
A typical CTG output for a woman not in labour. A: Fetal heartbeat; B: Indicator showing movements felt by mother (caused by pressing a button); C: Fetal movement; D: Uterine contractions
Assessment of how fetus will handle contractions of childbirth
Induce contractions with oxytocin or nipple stimulation to achieve 3 contractions (strength of 200+ Montevideo units) in 10 minutes
Assess for
Bradycardia: fetal heart rate less than 110 bpm
Decelerations:
Contraction stress test is positive if at least half the contractions are followed by late decelerations
Type
Timing and shape
Indicative of
Intervention
Early decel.
Mirrors contractions
Head compression
None
Variable
Abrupt, V-shaped, random relation to contractions
Cord compression
None unless recurrent
Late
Begin when contractions peak
Placental insufficiency
Immediate delivery
Combines NST with ultrasound measurements.
Score based on 5 criteria (2 pts each) for total of 1-10: (APGAR for fetus)
Defined as: diagnosis of diabetes 20 weeks gestation.
Risk factors: BMI 30; history of prediabetes; family hx of DM; age 25; history of stillbirth, polyhydramnios, macrosomia, hypertension, steroid use, PCOS
Diagnose as follows:
One hour glucose tolerance test: Give 50 g glucose, measure blood sugar at 1 hr
If above 140, proceed to three hour test
Three hour glucose tolerance test: Give 100 g glucose, measure blood sure at 0, 1, 2, and 3 hrs
If above 90, 190, 155, or 140, respectively, then diagnosis is gestational diabetes mellitus.
Other findings:
High glucose or prediabetes before pregnancy
High HbA1c
T1DM has anti-insulin or anti-islet cell antibodies
Treat GDM first with diet and exercise; postprandial insulin if refractory; and metformin and glyburide if insulin is contraindicated.
Premise: Alloimmunization is a concern if mom is Rh Ag negative and baby is Rh Ag positive. If there is blood mixing, she can develop anti-Rh antibodies. Her immune system can then attack Rh Ag positive fetus, causing fetal anemia.
To screen…
For Rh Ag negative mom, check for Rh antibodies
If mom is Rh antibody negative
If baby can be Rh Ag + (dad is + or unknown), use RhoGAM at 28 weeks and at delivery
If mom is Rh antibody positive (specifically for type D)
Perform transcranial doppler to assess for fetal anemia
High blood velocities can be indicative of fetal anemia (less viscous blood flows faster)
Consider intrauterine blood transfusion or early delivery (if after 36 weeks)
RhoGAM = Rho (D) Immune Globulin
Hgb = RBC mass / plasma volume
Screen moms at 28 weeks with CBC or H&H.
If Hgb 10 or Hct 30, perform iron studies
Iron def anemia: low ferritin, low MCV, high RDW
Most common cause of anemia in pregnancy
Add iron supplement (30 mg/day, which is a 100% increase)
Sampling of small amount of amniotic fluid through transabdominal needle aspiration; after 16 weeks
Used to diagnose NTDs and genetic disorders, including down’s syndrome
Risk: fetal loss (1/200 to 1/300); chorioamnionitis; fetal injury; alloimmunization; ROM
Replaced with quad screen (measure maternal proteins) and cell-free DNA (detect fetal DNA in mom’s circulation)
dilutional anemia
Ultrasound
Nonstress test
Contraction stress test
Biophysical profile
Diabetes screen
Rhesus screen
Anemia screen
Amniocentesis
Chorionic villus
sampling
Percutaneous umbilical cord blood sampling
Procedure: blood is collected from umbilical vein to detect fetal infections, fetal anemia, Rh sensitization, or chromosomal defects.
Performed after 18-20 weeks and before 34 weeks (for late detection)
For fetal anemia, perform transcranial Doppler to confirm
Unique benefit: creates vascular access; can transfuse baby → fix fetal anemia










Информация по комментариям в разработке