This is a brief video on somatic symptom and factitious disorders.
I created this presentation with Google Slides.
Images were created or taken from Wikimedia Commons
I created this video with the YouTube Video Editor.
ADDITIONAL TAGS:
Somatic symptom
and
factitious disorders
in the DSM-5
Somatic symptom disorder
Illness anxiety disorder
Conversion disorder
Factitious disorder
Malingering
Also/previously called somatoform disorder, somatization disorder
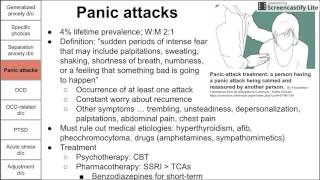
At least one somatic symptom (such as pain) along with excessive fear, worry, stress, or behavioral change regarding this pain
Duration of 6 months
Similar to illness anxiety in the fear/stress but with actual somatic symptoms
Symptom(s) is/are subconsciously driven; patients actually believe they has a disorder
EPI: F M; 5-7% prevalence; risk factors include low SES, low education, older age, unemployment
Prognosis: symptoms can get better or worse over time based on mood and/or stress
Patients often present frustrated having seen many doctors all not believing their symptoms with many negative workups
Management:
Acknowledge symptoms (because they are real)
Schedule regular follow-ups with a single PCP
Build rapport
Allows you to monitor any changes in symptoms
Avoid unnecessary workup and treatment
Somatic symptom disorder
Somatic symptom disorder
Illness anxiety disorder
Conversion disorder
Factitious disorder
Malingering
Also/previously called hypochondriasis, hypochondria, health anxiety
Excessive and undue fear, worry, stress, and/or behavioral change regarding having or being diagnosed with a serious illness
Duration of 6 months
Somatic symptoms are absent or very minor
Preoccupation with illness severely impacts their daily functioning
Sometimes caused by recent psychological stressor
Such as death in family → worry about same disease in self
Reassurance is often ineffective
Epi: M=F; ⅔ have another psychiatric illness; most prevalent in 20s-30s
Management:
Acknowledge concerns
Schedule regular follow-ups with a single PCP
Psychotherapy (CBT)
Screen for comorbid anxiety and depression, consider SSRI
If source is psychological stressor, resolve that stressor
Also called functional neurological symptom
Patient presents with at least one symptom (usually neurologic, such as numbness, blindness, mutism, or paralysis) that cannot be explained neurologically (not in normal stroke pattern)
Symptom onset is usually abrupt and following significant life stress or event (death of family member, bereavement)
Patient’s are often indifferent to or unconcerned with their symptom(s)
La belle indifference
Epi: WM; most frequent in adolescence and early adulthood
Pseudoseizures, or psychogenic nonepileptic seizures, can be the symptom of conversion disorder
Differentiate from epileptic seizure with prolactin level (elevated in epileptic) and EEG (normal in pseudoseizure)
Management:
Education about conversion disorder; reassurance that symptom will resolve
Consider CBT if symptoms persist
Spontaneous recovery usually occurs
Also known as Munchausen's syndrome when severe
Patient acts as if he has an illness by deliberately producing, feigning, or exaggerating symptoms, purely to attain a patient's role with no secondary gain or external reward
Patient often creates symptoms in dangerous ways, such as injecting themselves with feces (infection) or insulin (hypoglycemia) or ingesting blood and inducing vomiting (hematemesis)
Can also create less serious symptoms: abd pain, depression, hallucinations
Patient can present themselves as patient or present another as a patient (Munchausen’s by proxy)
Parent making child sick is child abuse
Epi: WM; higher incidence in healthcare workers
Management:
Confront in nonthreatening manner
Document and contact PCP and other providers to avoid unnecessary procedures
Patient fabricates symptoms of mental or physical disorders for secondary gain or external reward
Secondary gain is oftentimes getting out of work/school, obtaining drugs, clearing charges/legal record, free room and board, etc
Malingering is NOT a mental illness or psychiatric pathology
Oftentimes present as ill-defined, nonspecific complaints that don’t add up; often unsatisfied with reassurance or negative workup
Symptoms improve once secondary gain is achieved
Epi: MW; often in patients with antisocial personality disorder
Management:
Present the patient with discrepancies between objective findings and their subjective report
Give patient opportunity to admit malingering
Do not confront with hostility







Информация по комментариям в разработке