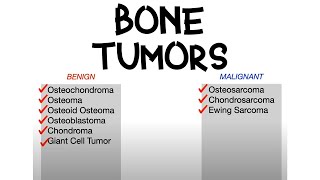
This is a brief video on benign and malignant neoplasms of hard tissues (bone and cartilage).
I created this presentation with Google Slides.
Images were created or taken from Wikimedia Commons
I created this video with the YouTube Video Editor.
ADDITIONAL TAGS:
Bone and cartilage tumors
Benign and malignant neoplasms of hard tissues
Osteoma
Osteoid osteoma
Osteochondroma
Nonossifying fibroma
Giant cell tumor
Chondroma /
Ecchondroma /
Enchondroma
Osteosarcoma
Ewing sarcoma
Chondrosarcoma
Benign
Malignant
Benign tumor of bone, typically the skull/facial bones
Can obstruct the nose or sinuses
Associated with Gardner’s syndrome
Familial adenomatous polyposis (large intestine polyps) with cancers outside the GI tract (thyroid, liver and kidneys)
Osteoma of the frontal sinus on CT
By Hellerhoff - Own work, CC BY-SA 3.0,
Osteoid osteoma
Benign bone-forming tumor
One of few tumors that occurs in the cortex (peripheral bone (vs central bone, medulla))
Occurs in diaphysis of bone
Radiography: mass of dense origin (nidus) and opaque cortical border of reactive, sclerotic bone
Reactive rim of sclerotic bone → benign
Mass is less than 2 cm in diameter
Clinical: bone pain, especially nighttime pain, with excellent relief with NSAIDs
Otherwise treat with radiofrequency ablation
Histo: immature-appearing bone, fibrovascular tissue, active osteoblasts and osteoclasts in nidus, no cellular atypia or mitotic figures
CT scan showing an osteoid osteoma of the fibula with a clearly visible nidus.
AKA fibroxanthoma, fibrous cortical defect (but larger)
Fibrous bone lesion → debateable if neoplasm or bone growth disorder
Occurs in cortex of bone
Epi: adolescents, young adults
Radiography: sharp borders, eccentric, lobulated/septated, around metaphysis against the cortex (usually of tibia or femur), with thin sclerotic rim of bone, with no periosteal reaction
Usually incidental finding
Histo: fibrous tissue (disorganized bunch of collagen) adjacent to normal bone, foam cells, whorled fibrous tissue
Treatment: no intervention required → naturally involutes spontaneously
Can cause pathologic fractures
Giant cell tumor
AKA GCToB, “osteoclastoma”
Tumor of osteoclast-like cells (multinucleated giant cells) and bone stromal cells
Arises from epiphyseal plate after closure, extends to articular surface (in epiphysis region); usually around knee
Benign but locally aggressive; 2% are malignant → often to lungs
Epi: age of 30s to 50s
Clinical: pain, swelling
Radiography: “soap bubble” appearance, radiolucent with no matrix calcification, no reactive sclerosis, no periosteal reaction, extends to cartilage through epiphysis
Histo: no atypia, giant cells look like elongated stromal cells with oval nuclei
Spreads aggressively locally
Treatment: curettage, grafting, and cementation or resection (lower recurrence but mechanical dysfunction)
Denosumab (RANKL inhibitor) might be effective
Benign tumors of cartilage with lobular growing pattern
Tumor cells resemble cartilage and produce cartilaginous matrix
Arises from medulla of long bones
Often occurs in long bones of hand/feet
Most common tumors of the hand
Chondroma is umbrella term containing ecchondroma and enchondroma
Enchondroma - tumor grows within the bone and expands it.
Central calcification within bone (medulla), no cortical breakthrough
Radiography: radiodense, “rings/arcs” “popcorn”, “snowflake”, stippled,
Often found incidentally → treatment: observation
Histo: bland, few cells, no atypia
Treatment: if painful, remove by curettage
Rare malignant transformation to chondrosarcoma (even rarer in hands and feet)
Osteosarcoma
AKA osteogenic sarcoma
Both osteoblastic and osteoclastic activity
Periosteal osteosarcoma is “stuck on” compared to osteochondroma
Poorly defined borders, no reactive rim → malignant
Histo: atypical, pleomorphic malignant spindle cells producing osteoid or bone
Ewing sarcoma
AKA Ewing’s sarcoma
Malignant tumor made of small round blue cells (poorly differentiated cells)
Bone destruction in diaphyseal or meta-diaphyseal location
Caused by t(11:22) translocation → fusion protein EWS-FLI 1
11+22=33, Patrick Ewing’s NBA number
Uncertain origin (likely neuroectodermal)
Epi: teens (15 years old) and young adults; M:F 1.6:1
Clinical: increased WBCs, increased erythrocyte sedimentation rate
Look like neuroblastoma, lymphomas
Responsive to chemo, esp combined with radiation
of cartilage
Slow growing, but grow
Most often affects axial/central skeleton (ie, pelvis, spine, scapula), otherwise in metaphysis, arising in medulla
some areas of necrosis
Treatment: surgical resection or amputation
No response to chemotherapy or radiation









Информация по комментариям в разработке